Diverticulosis is one of the most common benign changes in the colon. The diverticula usually occur in the sigmoid colon, which is also known as sigmoid diverticulosis. Only in about 10-20% of those affected does the diverticulum become inflamed. Sigmoid diverticulitis is treated conservatively or surgically, depending on the degree of severity.
Diverticula can occur in several sections of the intestine, primarily in the colon. If the clinical symptoms are dominated by pain localized in the left lower abdomen, inflammatory diseases of the sigmoid colon are at the forefront of the causes [1,2,6,7]. Acute and chronic courses are possible. Ischemic proctosigmoiditis is a rarer clinical picture with similar symptoms.
Colonic diverticula occur more frequently with increasing age and are usually asymptomatic. A connection between a frequent diet of red meat, nicotine abuse and obesity is suspected. Prolonged treatment with non-steroidal anti-inflammatory drugs, paracetamol, corticosteroids and opioids can also predispose to diverticulosis. A sex predisposition is not known. Stool retention in diverticula can lead to the invasion of intestinal bacteria and inflammatory mucosal ulcerations due to obstruction of the diverticular neck. These changes occur more frequently in the sigmoid colon.
The pain symptoms, sometimes colicky, are predominantly in the left lower abdomen, corresponding with fever and increased inflammatory parameters. Nausea, diarrhea and constipation may also occur. Almost 70% of people over the age of 70 have diverticulosis, 10-25% of patients suffer from diverticulitis. Known complications are covered or free perforation, inflammatory stenosis of the intestinal segment and fistula formation in neighboring organs.
On clinical examination, a painful roller in the left lower abdomen is often conspicuous.
Complicated diverticulitis is an indication for surgery, even with antibiotic treatment. Minimally invasive methods are increasingly being used [4]. Two-stage surgical treatments have also been used successfully for covered perforation [3].
X-ray examinations are limited in their significance for this question [7]. The colon double contrast examination frequently used before the era of cross-sectional imaging was able to detect diverticula in free diverticular necks, but the inflammatory alteration often escaped visual detection.
Sonography is the first step in the diagnostic cascade [5,7]. Typically in diverticulitis, low-echo, sometimes partially air-filled nodules can be seen next to the intestinal wall. Segmental intestinal wall thickening with stenosis of the lumen can be visualized. The surrounding fatty tissue is echogenically altered. If an abscess or perforation cannot be ruled out sonographically, computed tomography with intravenous injection of contrast medium should be performed immediately. This examination modality provides the most comprehensive information about the extent of the inflammation, the parenchymal and hollow organs in the vicinity and the surrounding retroperitoneal structures.
Computed tomography shows distended diverticula and localized thickening of the bowel wall, eccentric or circular [7]. The adjacent paracolic fatty tissue is inflammatory dense. Intramural gas inclusions or contrast media can be indications of an initial fistula. Soft tissue lymphysema can be detected in the abdominal or thoracic wall. With enterovesical fistula, air is present in the urinary bladder. Colonoscopy supplements the computed tomography information [2].
Magnetic resonance imaging has also become a valuable tool in intestinal diagnostics. Multiplanar sequences without and with fat saturation and also with contrast enhancement can reliably detect sigmoid diverticulosis and sigmoiditis [6]. An advantage over CT is the lack of radiation exposure, a disadvantage is the longer examination time and higher susceptibility to artifacts as well as pacemakers as a contraindication, especially in the older patient clientele.
Case study
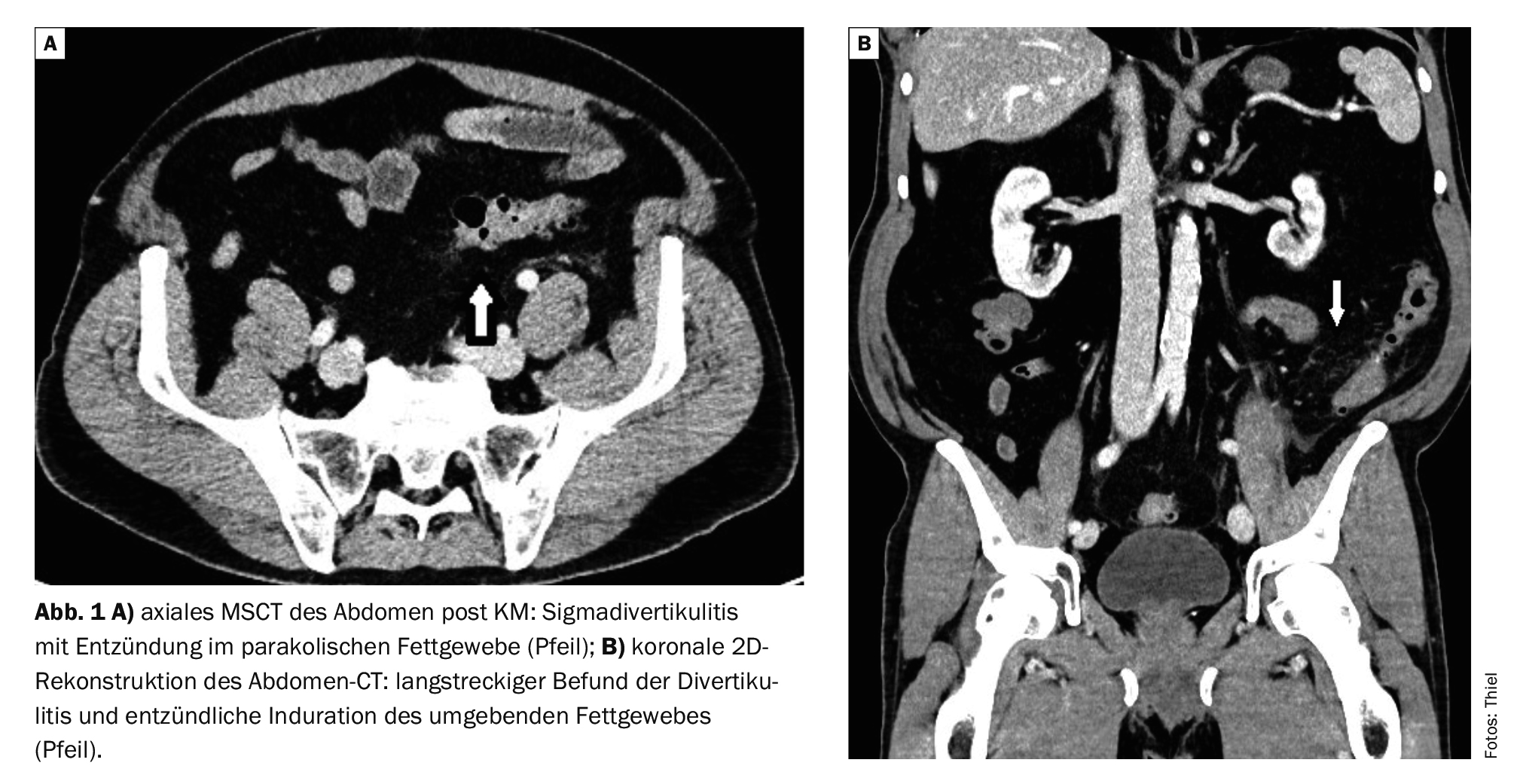
In case example 1, a 59-year-old patient had recurrent episodes of diverticulitis, primarily in the descending colon and sigmoid colon (Fig. 1A and 1B) . A clear edematous paracolic inflammation of the fatty tissue is detectable as a sign of the acute inflammatory stage. There was no evidence of perforation or abscessation.
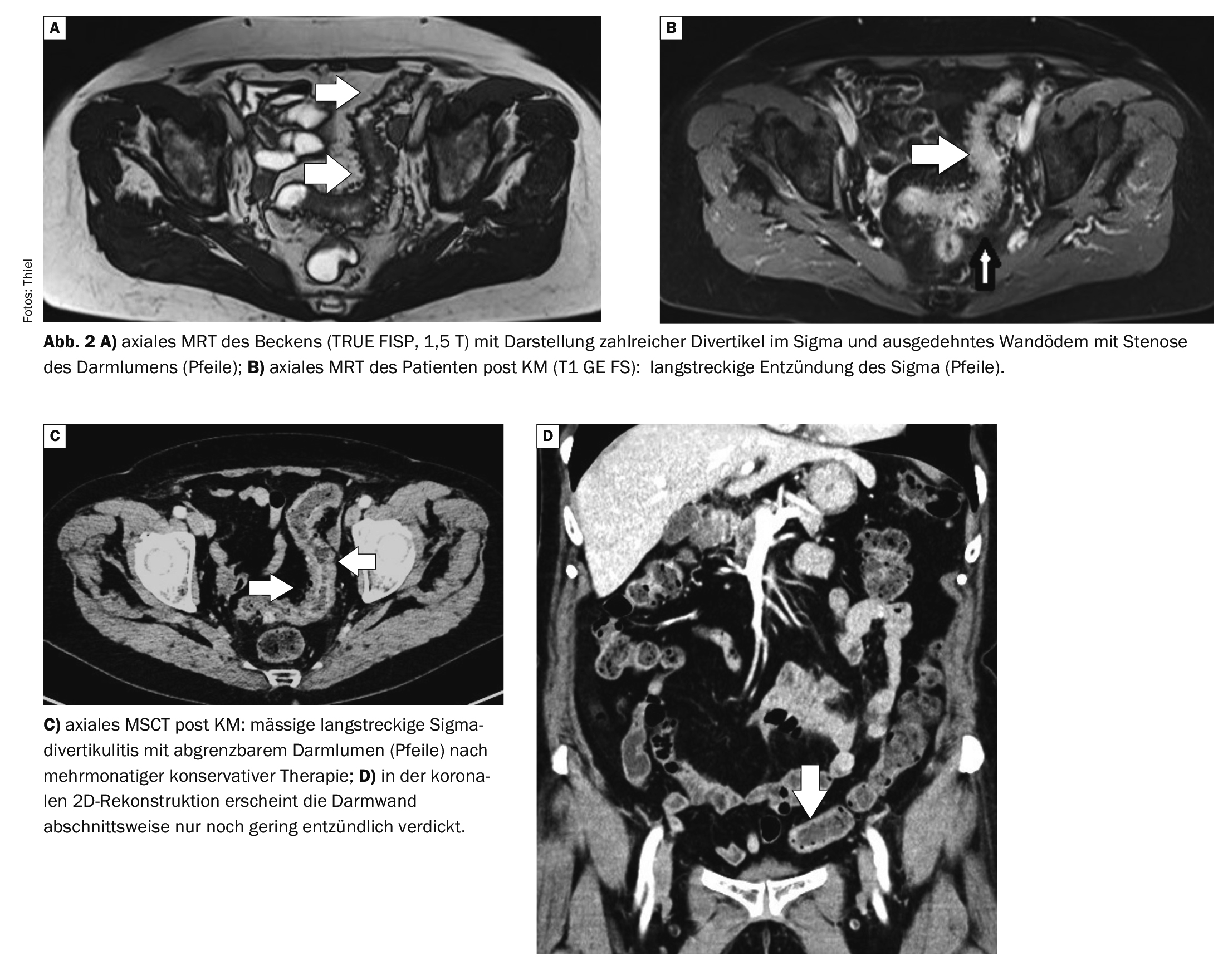
Case 2 demonstrates the course of sigmoid diverticulitis in a 70-year-old female patient (Fig. 2A to 2D) . The initial MRI of the abdomen showed a prolonged inflammation of the sigmoid colon with extensive diverticulitis; the intestinal lumen was considerably stenosed. At a check-up after intensive conservative therapy, an improvement was seen in the CT scan, with wall swelling still visible, the bowel lumen was still moderately stenosed. Fistula formation or abscessation could be ruled out.
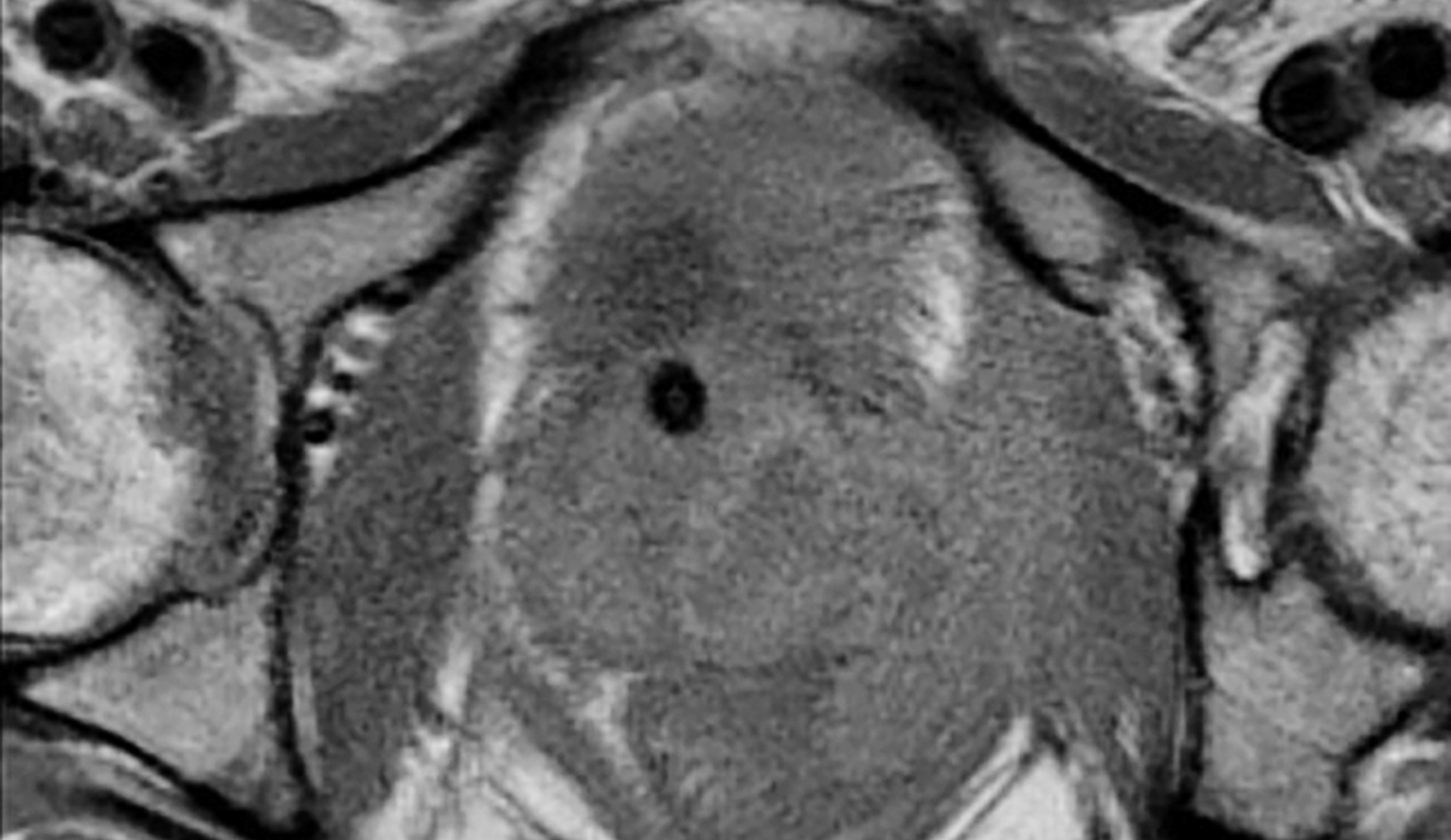
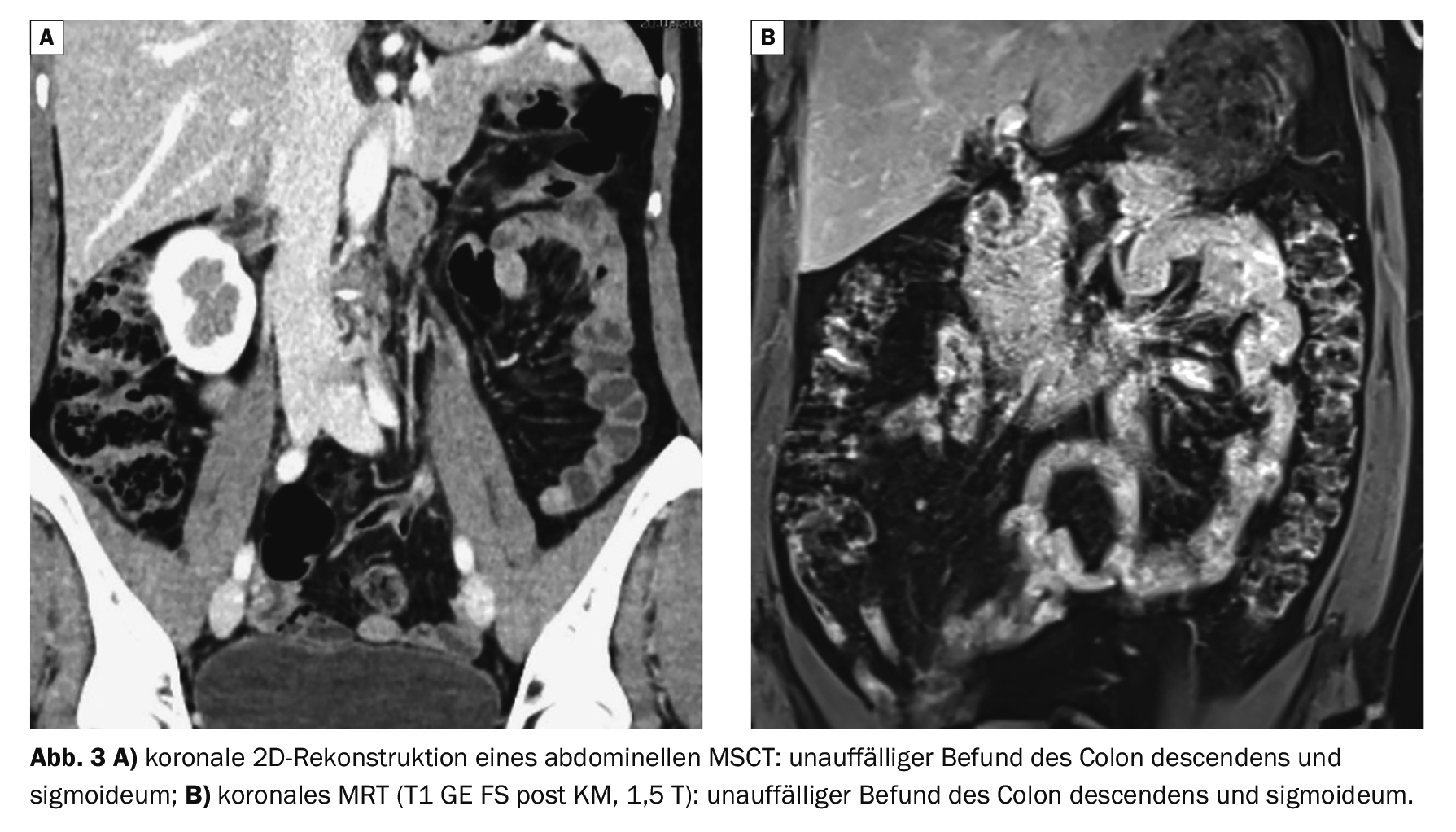
Case study 3 shows normal findings of the sigmoid colon on CT (Fig. 3A) and MRI (Fig. 3B) for comparison.
Take-Home-Messages
- Diverticulosis is a relatively common intestinal disease that occurs more frequently with increasing age.
- Diverticulitis occurs primarily in the area of the sigmoid colon.
- Typical symptoms are pain in the left lower abdomen, also fever
- and inflammatory laboratory constellations.
- In mild cases, conservative drug therapy is the first choice; predisposing factors should be excluded.
- In the event of complications with perforation or abscessation, surgical treatment is required.
Literature:
- Antwerpes F, et al.: Divertikulitis. https://flexikon.doccheck.com/de/Divertikulitis, (last accessed 28.05.2024).
- Baum JA, Companoni RAC: Divertikulitis. www.msdmanuals.com/de-de/heim, (last accessed 28.05.2024)
- Claas S, Traska T: Perforierte Sigmadivertikulitis als Ursache einer akuten nekrotisierenden Fasziitis. Zentralbl Chir 2011; 136-P_03.
- «Sigmadivertikulitis», https://chi.charite.de/leistungen/allgemeine_bauchchirurgie/sigmadivertikulitis, (last accessed 28.05.2024).
- «Divertikulitis», https://sonographiebilder.de/divertikulitis, (last accessed 28.05.2024)
- Piroth W, et al.: Bildgebende Diagnostik der Sigmadivertikulitis. Dtsch Arztebl 2007; 104(49): A-3400/B-2989/C-2885.
- Wiesner W, Kirchhoff TD, Opherk JP: Differenzialdiagnose des akuten Abdomens (Teil II). Radiologie up2date 1; 2009; 35–45.
HAUSARZT PRAXIS 2024; 19(6): 48–50